
Regulations Amending the Canada Student Loans Regulations and the Canada Student Financial Assistance Regulations: SOR/2024-210
Canada Gazette, Part II, Volume 158, Number 23
Registration
SOR/2024-210 October 25, 2024
CANADA STUDENT LOANS ACT
CANADA STUDENT FINANCIAL ASSISTANCE ACT
P.C. 2024-1136 October 25, 2024
Her Excellency the Governor General in Council, on the recommendation of the Minister of Employment and Social Development, makes the annexed Regulations Amending the Canada Student Loans Regulations and the Canada Student Financial Assistance Regulations under section 17footnote a of the Canada Student Loans Act footnote b and subsection 15(1)footnote c of the Canada Student Financial Assistance Act footnote d.
Regulations Amending the Canada Student Loans Regulations and the Canada Student Financial Assistance Regulations
Canada Student Loans Act
Canada Student Loans Regulations
1 The definition under-served rural or remote community in subsection 2(1) of the Canada Student Loans Regulations footnote 1 is replaced by the following:
- under-served rural or remote community
- means a population centre with a population of no more than 30,000 based on data published in the most recent census of population or a rural area, based on data published in that census. (collectivité rurale ou éloignée mal desservie)
2 Section 17 of the Regulations is replaced by the following:
17 Sections 18 and 19 apply to a borrower who does not have any outstanding student loans under the Canada Student Financial Assistance Act.
3 (1) Paragraph 19(1)(a) of the Regulations is replaced by the following:
- (a) either
- (i) have begun to work as a family physician, nurse or nurse practitioner in an under-served rural or remote community during the year, or
- (ii) have continued during the year to work as a family physician, nurse or nurse practitioner in a community in respect of which the borrower qualified for loan forgiveness for the previous year; and
(2) Section 19 of the Regulations is amended by adding the following after subsection (2):
(3) For the purposes of subsection (1), the results of a census of population apply six months after the day on which the census is published by Statistics Canada or on the November 1 following that day, whichever is later.
Canada Student Financial Assistance Act
Canada Student Financial Assistance Regulations
4 The definition under-served rural or remote community in subsection 2(1) of the Canada Student Financial Assistance Regulations footnote 2 is replaced by the following:
- under-served rural or remote community
- means a population centre with a population of no more than 30,000 based on data published in the most recent census of population or a rural area, based on data published in that census. (collectivité rurale ou éloignée mal desservie)
5 Section 27 of the Regulations and the heading “Application” before it are repealed.
6 (1) Paragraph 29(1)(a) of the Regulations is replaced by the following:
- (a) either
- (i) have begun to work as a family physician, nurse or nurse practitioner in an under-served rural or remote community during the year, or
- (ii) have continued during the year to work as a family physician, nurse or nurse practitioner in a community in respect of which the borrower qualified for loan forgiveness for the previous year; and
(2) Section 29 of the Regulations is amended by adding the following after subsection (2):
(3) For the purposes of subsection (1), the results of a census of population apply six months after the day on which the census is published by Statistics Canada or on the November 1 following that day, whichever is later.
Transitional Provisions
7 An under-served rural or remote community as defined in subsection 2(1) of the Canada Student Loans Regulations immediately before the day on which these Regulations come into force continues to be an under-served rural or remote community for the purposes of section 19 of those Regulations until November 1, 2027 or the day that is 6 months after the day on which a census is published by Statistics Canada, whichever is later.
8 An under-served rural or remote community as defined in subsection 2(1) of the Canada Student Financial Assistance Regulations immediately before the day on which these Regulations come into force continues to be an under-served rural or remote community for the purposes of section 29 of those Regulations until November 1, 2027 or the day that is 6 months after the day on which a census is published by Statistics Canada, whichever is later.
Coming into Force
9 These Regulations come into force on the day on which they are published in the Canada Gazette, Part II.
REGULATORY IMPACT ANALYSIS STATEMENT
(This statement is not part of the Regulations.)
Executive summary
Issues: Among the many factors that contribute to the limited access to health care services in rural and remote areas is the challenge of attracting family physicians, family medicine residents, nurses and nurse practitioners (doctors and nurses) to these communities. The Canada Student Loan forgiveness benefit (the forgiveness benefit) was put in place to help incentivize doctors and nurses to work in rural and remote communities. The current definition of an “under-served rural or remote community” tends to exclude areas that may be considered rural within broader municipalities, making them ineligible for the benefit despite being small, under-served communities. A revised definition will address a Government of Canada Budget 2023 commitment to ensure that certain communities in need are not excluded from the forgiveness benefit.
Description: Amendments to the Canada Student Financial Assistance Regulations and the Canada Student Loans Regulations will change the definition of an “under-served rural or remote community” for the forgiveness benefit for doctors and nurses. Under the regulatory amendments, all areas considered rural areas by Statistics Canada will be eligible for the forgiveness benefit, as will the population centres of 30 000 or fewer (as defined by Statistics Canada in the Census Dictionary, and as determined by the most recent census of population).
Rationale: With the current shortage of health professionals in all of Canada, particularly in rural communities, these modifications will provide financial incentives for doctors and nurses to relocate to under-served areas by ensuring more rural communities are eligible for this benefit.
The amendments will expand the area of eligibility for the forgiveness benefit to include all rural areas and communities with populations of 30 000 or fewer. The change in definition is expected to initially increase the availability of health care services for approximately 1.7 million Canadians living in newly eligible areas. It is expected that this measure will incentivize 935 doctors and nurses to provide health services to a rural or remote community over a 10-year period. Literature suggests that this increase in the number of doctors and nurses in rural or remote regions will result in better health outcomes in rural and remote areas of Canada.
The cost of the amendments amounts to $87.4 million (present value) over 10 years. This includes costs for the federal government to provide additional loan forgiveness in newly eligible areas as well as costs for future borrowers in existing communities who will not be eligible for the forgiveness benefit after 2027–2028. Given improved access to health services and, as suggested by the evidence in the literature reviewed, better health outcomes, the benefits to Canadians living in both rural and remote communities outweigh the costs of implementing the regulatory amendments.
Issues
Among the many factors that contribute to the limited access to health care services in rural and remote areas is the challenge of attracting family physicians, family medicine residents, nurses and nurse practitioners (doctors and nurses) to these communities. The Canada Student Loan forgiveness benefit (the forgiveness benefit) was put in place to help incentivize doctors and nurses to work in rural and remote communities. The current definition of an “under-served rural or remote community” tends to exclude areas that may be considered rural within broader municipalities, making them ineligible for the benefit despite being small, under-served communities. A revised definition will address a Government of Canada Budget 2023 commitment to ensure that certain communities in need are not excluded from the forgiveness benefit.
Background
Canada Student Financial Assistance Program
The Canada Student Financial Assistance Program (the Program or the CSFA Program) provides eligible students with Canada Student Loans (loans), as well as non-repayable Canada Student Grants (grants) to help them pay for post-secondary education at a designated college, university or other post-secondary institution. Grants and loans are available to students from nine participating provinces — British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, New Brunswick, Nova Scotia, Newfoundland and Labrador, Prince Edward Island — and the Yukon. In these jurisdictions, students receive both federal and provincial/territorial (P/T) student aid. Meanwhile, Quebec, Nunavut and the Northwest Territories have opted out of the Program and receive alternative payments from the Government of Canada to administer their own student financial assistance programs.
Since 2013, to expand the provision of primary health care services to more Canadians in under-served geographical areas, the Government of Canada has provided a loan forgiveness benefit to doctors and nurses who practise in rural and remote communities. This benefit enables these rural and remote communities to attract and retain health care providers,footnote 3 thus increasing access to health care in these areas. As of November 3, 2023, doctors are eligible for federal loan forgiveness of up to $60,000 over five years, and nurses are eligible for federal loan forgiveness of up to $30,000 over five years.
According to the Program’s statistics, the greatest amount of loan forgiveness between fiscal year 2017–2018 and fiscal year 2021–2022 was granted to registered nurses ($56.8 million [M]), followed by family medicine residents ($24M), licensed practical nurses ($13.7M) and family physicians ($10M).
The eligibility conditions for the forgiveness benefit are prescribed under section 29 of the Canada Student Financial Assistance Regulations footnote 4 and section 19 of the Canada Student Loans Regulations.footnote 5 In order to receive the forgiveness benefit, a borrower must have worked in an “under-served rural or remote community,” as a doctor or nurse during the previous year, and must have applied for loan forgiveness no later than 90 days after the end of that year.
Subsection 2(1) of the Canada Student Financial Assistance Regulations and the Canada Student Loans Regulations defines an “under-served rural or remote community” as any census subdivision (defined in the Statistics Canada document entitled Standard Geographical Classification 2011footnote 6 that does not have census tracts and is located outside the capitals of the 10 provinces. Census tracts are described in the Standard Geographical Classification 2011 as elements that exist in all census metropolitan areas and in census agglomerations with a core population of 50 000 or more.footnote 7 To be eligible for the forgiveness benefit, the borrower must have worked in a community that meets these criteria, which in general means a community with 50 000 people or fewer.
Census metropolitan areas and census agglomerations can cover a large territory and include rural areas that are within the boundaries of larger municipalities. When determining the areas included in census metropolitan areas and census agglomerations, Statistics Canada does not consider population density. Instead, it considers whether the area in question is integrated with the urban core, using commuting flows derived from previous census place of work data. Because of this, certain small under-served rural communities where residents commonly commute to urban centres may not be covered by the forgiveness benefit. While some individuals living in rural areas may be willing to commute long distances to access health services, many who require health services, especially an older population, may not be as mobile. For example, the municipality of Halifax amalgamated the rural areas surrounding it, encompassing over 5 000 km2. Translated into commuting distance, this requires residents of Sheet Harbour (an area within the agglomeration) to drive over one and a half hours to reach downtown Halifax. Due to the current definition of an “under-served rural or remote community,” low-population areas distant from Halifax, but within the agglomeration, such as Sheet Harbour, are ineligible for the forgiveness benefit.
Another problem with the current definition is that it is based on data from the 2011 census. This means that a community that was under the population threshold at that time will remain eligible for the forgiveness benefit indefinitely, regardless of population growth. As an example, Fort McMurray, Alberta, is eligible for the forgiveness benefit based on the current definition, despite having a population of over 68 000 in the 2021 census of population.
In Budget 2023, the Government of Canada committed to encouraging more doctors and nurses to practise in under-served rural and remote communities. Specifically, Budget 2023 committed to expanding the reach of the forgiveness benefit to more rural communities, including all communities with populations of 30 000 or fewer.
Objective
The objective of these regulatory amendments is to ensure that doctors and nurses working in all rural areas and population centres with a population of 30 000 or fewer are eligible for loan forgiveness. This is expected to incentivize doctors and nurses to move to these communities which, in turn, is expected to result in better access to health care for residents of under-served rural and remote communities.
Description
The regulatory amendments will replace the existing definition of “under-served rural or remote community,” which currently references “census subdivisions” and “census tracts,” as defined by Statistics Canada, and relies on 2011 census population data. The new definition of “under-served rural or remote community” references Statistics Canada’s definitions of both “rural areas” and “population centres” (restricted to population centres of 30 000 or fewer) and relies on the most recent census population data, as they are published.
More specifically, “population centres” are defined in Statistics Canada’s Census Dictionary as having a population of at least 1 000 and a population density of 400 persons or more per square kilometre. “Rural areas” are defined in the same document as all areas outside population centres. Taken together, population centres and rural areas cover all of Canada. With these amendments, smaller communities that are within the boundaries of larger municipalities will become eligible for the benefit. Integrating the concept of population centres also promotes alignment with other legislation, such as the Bank Act and the Income Tax Act, which use Statistics Canada’s definition of population centres to define eligibility for certain programs.
The change in definition will result in over 200 communities being added to the list of areas where doctors and nurses can qualify for the forgiveness benefit. It will also result in approximately 25 communities losing eligibility, as their populations in the most recent census of population (2021) are larger than 30 000.
The regulatory amendments include a transitional provision, which provides that communities eligible for the forgiveness benefit under the current regulations will retain eligibility until the 2026 census.
The maps below illustrate the impact of the revised definition on the area of Halifax, Nova Scotia, and Sudbury, Ontario.
Figure 1: Halifax, Nova Scotia — Current definition
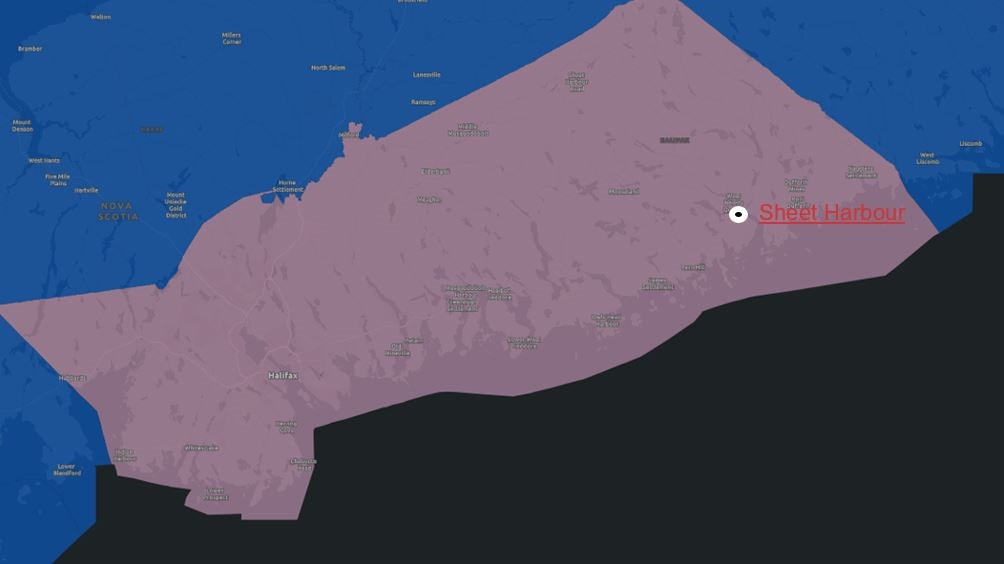
Figure 1: Halifax, Nova Scotia — Current definition - Text version
Halifax area, indicating the Halifax Census Metropolitan Area which is ineligible under the current definition. The location of Sheet Harbour is indicated, which is included in the ineligible area.
Red area: Halifax census metropolitan area, including Sheet Harbour, ineligible under current definition.
Surrounding area: Eligible under current definition.
Figure 2: Halifax, Nova Scotia — Revised definition
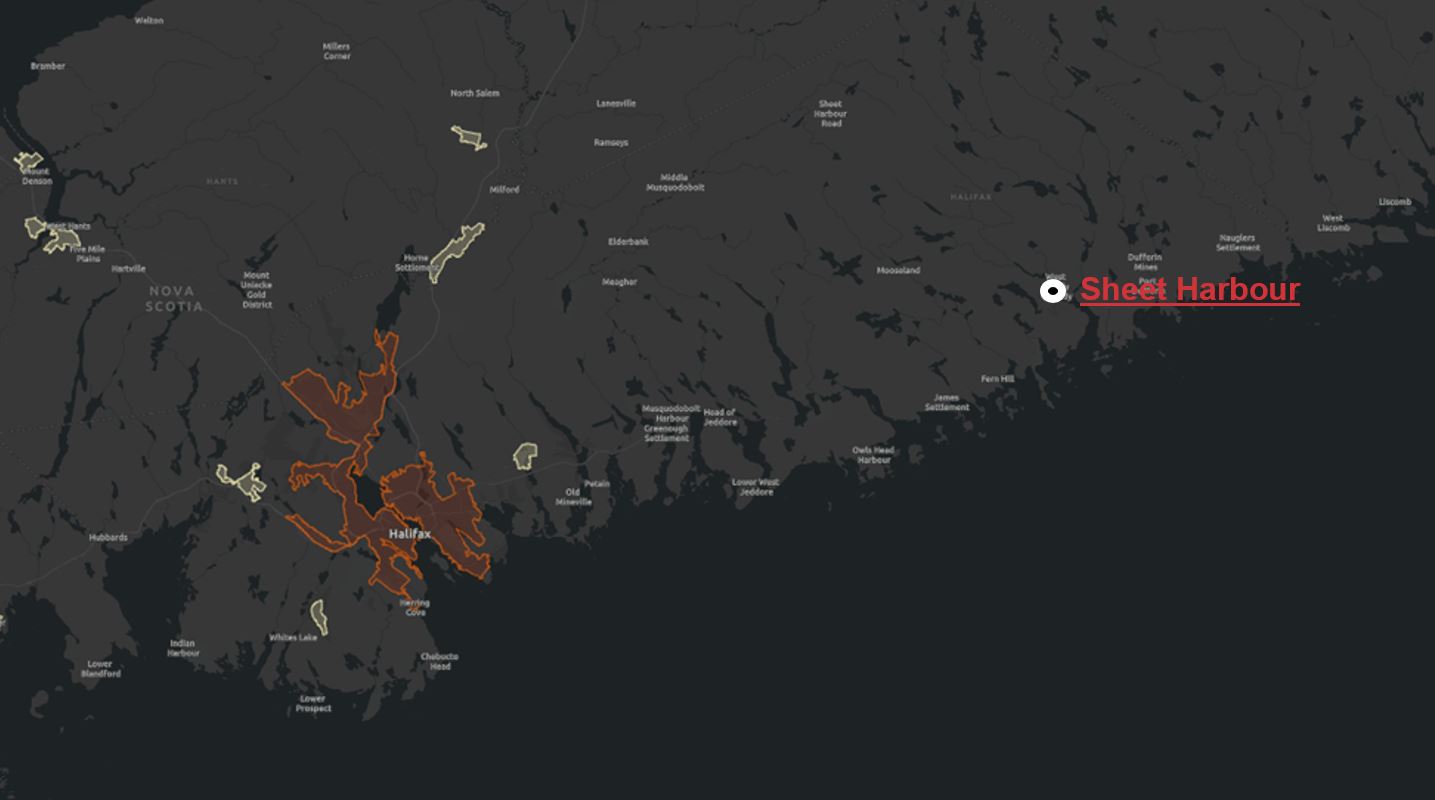
Figure 2: Halifax, Nova Scotia — Revised definition - Text version
Halifax area, indicating the population centre of Halifax, which would remain ineligible under the proposed definition. The location of Sheet Harbour is indicated, which is in an eligible area.
Orange area: Population centre of Halifax — only area that remains ineligible.
Yellow areas: Small population centres (population of fewer than 30 000) are now all eligible.
Other areas: Rural areas, as defined by Statistics Canada’s population centre definition, include Sheet Harbour, are now all eligible.
Figure 3: Sudbury, Ontario — Current definition

Figure 3: Sudbury, Ontario — Current definition - Text version
Sudbury area, indicating the Greater Sudbury / Grand Sudbury Census Metropolitan Area which is ineligible under the current definition.
Red area: Greater Sudbury / Grand Sudbury census metropolitan area, ineligible under current definition.
Surrounding area: Eligible under current definition.
Figure 4: Sudbury, Ontario — Revised definition
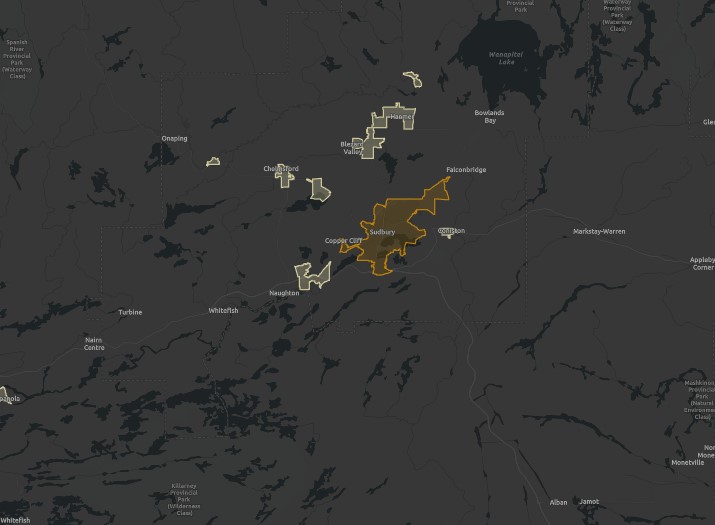
Figure 4: Sudbury, Ontario — Revised definition - Text version
Sudbury area, indicating the population centre of Sudbury, which would remain ineligible under the proposed definition.
Orange area: Population centre of Sudbury — only area that remains ineligible.
Yellow areas: Small population centres (population of less than 30 000) are now all eligible. New population centres becoming eligible under the revised definition include Coniston, Lively, Azilda, Chelmsford, Dowling, Valley East and Capreol.
Other areas: Rural areas, as defined by Statistics Canada are now all eligible.
Under the regulatory amendments, all borrowers who continue to work as a doctor or nurse in a community for which they received the forgiveness benefit the previous year will continue to receive the full benefit regardless of whether the eligibility of the community changes. The table below illustrates how this would work for a community called Town A. Town A has a population of 25 000 in the 2031 census and is therefore eligible for the forgiveness benefit. In the 2036 census, published in February 2037, it has a population of 32 000, and is no longer eligible.
| Example name | Year started working in Town A | Continues to work in Town A for 5 years? | Eligible for the full 5-year term of the forgiveness benefit? | Explanation |
|---|---|---|---|---|
| Sarah | 2035 | Yes | Yes | Although Town A will lose its eligibility for new applicants after the 2036 census, Sarah will remain eligible since, when she started working in Town A, it was eligible. |
| Charles | 2036 | No. In 2037, he moves to practice in Town B for a year before returning to Town A in 2038. | No | When Charles returns to Town A, his eligibility will be reassessed based on the latest census population size (32 000). |
| Masoud | 2038 | Yes | No | When Masoud starts working in Town A, it is not an eligible community based on the latest census. |
For the purposes of the loan forgiveness benefit, the regulatory amendments deem the results of a census of population to take effect six months after the day on which the census is published by Statistics Canada, or on November 1 following that day, whichever is later. This provision will provide predictability for stakeholders regarding changes in community eligibility. Census results have typically been published in February of the following year (e.g. census 2021 population data was published on February 9, 2022), in which case the results would always take effect for the forgiveness benefit on November 1. However, the Program needs at least six months to integrate eligibility changes. If, in the future, the census of population is not published in February, the regulatory provision ensures adequate time for changes to be implemented and for affected communities to consider their approaches to recruitment and retention (for example a community could advertise a deadline before which eligible doctors and nurses could begin practising in their community and still be eligible for the benefit).
Regulatory development
Consultation
Stakeholder tables
The Program regularly engages with stakeholders, including student groups and the provinces and territories, through the National Advisory Group on Student Financial Assistance (NAGSFA) and the Intergovernmental Consultative Committee on Student Financial Assistance (ICCSFA). In addition, for this measure, the Program also reached out to P/T health ministries with the support of Health Canada and the Federal-Provincial/Territorial (F-P/T) Committee on the Health Workforce. The F-P/T Committee on the Health Workforce reports to the F-P/T Conference of Deputy Ministers. Membership consists of the federal and provincial co-chairs plus one senior-level delegate from each federal, provincial and territorial Ministry of Health. Its mandate includes providing policy and strategic advice to the Conference of Deputy Ministers on health workforce issues and identifying emerging issues in the health workforce and health delivery.footnote 8 From May 17 to May 18, 2022, the Program met with stakeholders from NAGSFA and the Policy Development Sub-Committee under ICCSFA and advised that the definition of “under-served rural or remote community” was being reviewed. Feedback from these stakeholder tables supported a revised definition of “under-served rural or remote community” that could enable more borrowers working in under-served communities to access loan forgiveness. One NAGSFA member commented that there is currently confusion among students about the definition of “under-served rural or remote community” and noted differences between federal and provincial/territorial definitions. They signalled the federal plan to amend the definition of “under-served rural or remote community” would be an opportunity to reduce confusion.
On May 31, 2022, the Program met with P/T ministries of health through the F-P/T Committee on Health Workforce. At the meeting, some P/T health ministry representatives commented that the loan forgiveness benefit may be of limited use for physicians, given their higher pay after graduation and the need for additional loans through lines of credit while in medical school. Representatives also highlighted the shortage of health care professionals in rural and remote regions and noted the existence of a strong competitive appeal for doctors in the private sector to work in urban centres. However, the Committee did not provide insights on an approach to solve the shortage in rural, remote, and under-served communities. In addition, one stakeholder commented on the potential challenges of retaining health professionals after the loan forgiveness period ends under the forgiveness benefit.
The Program met bilaterally with officials from Health Canada, Innovation, Science and Economic Development Canada and Statistics Canada between April and August 2022. There was general support for enhancements to the forgiveness benefit during meetings with these federal colleagues.
Officials from Health Canada indicated they were aware of the issue of under-served rural and remote communities and the need for outlined the extent to which health care professionals in remote and rural communities, noting the complexity of this long-standing issue.
Innovation, Science and Economic Development Canada uses a variety of definitions for remote and rural communities, depending on the specific aim of a particular program.
Officials from Statistics Canada provided information related to geographic terms they use: census metropolitan areas and census agglomerations;footnote 9 population centres;footnote 10 and population density.footnote 11
Statistics Canada indicated that census metropolitan areas and census agglomerations are terms which include nearby areas within commuting distance. As a result, certain amalgamated municipalities contain smaller rural communities that are currently ineligible for the forgiveness benefit due to historical amalgamations. Population centres, which are defined as having a population density of at least 400 people per square kilometre and a population of 1 000 or more, are more focused areas compared to census metropolitan areas and census agglomerations.
Population density by itself was also considered by the Program as a way to define “under-served rural or remote areas,” but was rejected, as under-served rural and remote communities can often have clustered housing. This can lead to communities that have intense pockets of density despite a low population becoming ineligible. The population centre definition addresses this issue by also considering the population of the area along with its density.
Fall 2022 engagement
In fall 2022, the Program also engaged stakeholders on Budget 2022 commitments respecting the forgiveness benefit. These commitments included increasing the maximum amount of loan forgiveness by 50% for eligible doctors and nurses working in under-served rural and remote communities, expanding the list of eligible occupations, and reviewing the definition of “under-served rural or remote community.”footnote 12 As part of the engagement, a discussion paper and a questionnaire were sent out to 102 stakeholders.
Input was received from the following stakeholders: professional associations representing physicians and nurses, P/T health ministries, organizations representing the community interests of rural and remote communities, Indigenous stakeholders and NAGSFA and ICCSFA members. These groups represent 75 of the 102 stakeholders invited to provide input as part of the fall 2022 engagement. However, not all stakeholders that submitted responses addressed the question of changing the definition of “under-served rural or remote community.” Some left sections blank or indicated that their organization opted to not provide a perspective given this was not their area of expertise. In total, 9 responses were received from these 75 stakeholders discussing a revised definition for “under-served rural or remote community.” While the engagement was for three proposed changes to the forgiveness benefit, only feedback related to amending the definition of “under-served rural or remote community” is discussed below.
Stakeholders were asked to indicate rural or remote areas in Canada that are under-served with respect to access to medical services, but are not currently eligible for the forgiveness benefit.
Eight stakeholders identified a gap in the current definition and provided the following locations and groups that should be included in a new definition: Six Nations of the Grand River, all First Nations and Indigenous communities, northern communities (including northeast/western Ontario), Lethbridge (Alberta), Medicine Hat (Alberta), Fort St. John (Alberta), Charlottetown (Prince Edward Island), Summerside (Prince Edward Island) and Halifax (Nova Scotia). They also raised concerns that large, amalgamated municipalities could include communities that would otherwise be considered rural, remote, and under-served.
Out of six stakeholders that provided responses on the current Statistics Canada definitions of population centres and rural areas, two agreed with the definition. One organization advised that a community’s distance from an urban core should be considered in the definition, and another suggested that the definition should consider the level of unmet health care needs. Two provinces provided their own definitions of rural/remote communities for context, but they were not applicable on a federal scale.
In response to the inquiry of what should be the maximum population sizes for a rural and remote community to be eligible, one stakeholder responded that a population size of 15 000 or fewer should be considered, while another suggested that a population size of 150 000 or fewer should be considered.
In addition to the responses related to the appropriate definition of “under-served rural or remote community,” some stakeholders offered further insights. For example, one professional association representing physicians advocated for comprehensive student loan debt relief to support the retention of health care workers in areas of urgent need, including rural and remote areas. They supported increasing the supply of health professionals in rural and remote communities to help with retention, by reducing burnout and high staff turnover. They advised that many physicians leave isolated communities because of overwork and burnout. Under-resourcing in rural and remote areas was seen as a self-perpetuating problem leading to high staff turnover and heavy workloads for existing staff.
As well, one NAGSFA member and three provinces also suggested there was a lack of awareness of the benefit and an absence of coordination between F-P/T governments. The Program anticipates it would use existing stakeholder tables (e.g. ICCSFA, NAGSFA, F-P/T Committee on Health Workforce) to raise awareness of the changes to the forgiveness benefit and to foster greater collaboration with its P/T partners.
Results from the 2020 survey of forgiveness benefit recipients
In fall 2020, a survey was conducted with all recipients of the forgiveness benefit between 2013 and 2019. The survey, which received a 10% response rate (representing 232 doctors and 1 107 nurses), had the following objectives:
- To understand the effectiveness of the forgiveness benefit at recruiting health care professionals to work in under-served rural and remote communities; and
- To understand the extent to which recipients are satisfied with the Program and how it could improve.
The survey asked forgiveness benefit recipients about their experience with the benefit as well as their experience with working in under-served rural and remote communities. For example, the survey asked about debt and salary levels, amounts forgiven through the benefit, the reasons why a beneficiary chose to work in an eligible community, and questions about the ease of the application process and reasonableness of the benefit requirements.
Survey respondents revealed the forgiveness benefit contributed to their decision to work in under-served rural and remote communities, with respondents indicating that eligibility for the benefit represented approximately 30% of their decision-making in choosing to practice in a rural or remote community. However, respondents indicated that loan forgiveness was only one factor in their decision, with other strong influences, including their preference to live in a rural or remote area (35% of decision-making) and the fact that they have ties with family and friends in the community (31% of decision-making).
Furthermore, the survey found the forgiveness benefit may have a lasting positive impact on the retention of health professionals in under-served communities, with a combined total of 69% of respondents continuing to work in designated communities once they were no longer eligible for the benefit.
More than 9 in 10 recipients indicated they believed the eligibility requirements were reasonable. Among the minority of recipients who indicated that eligibility requirements are not reasonable, this was primarily attributed to a perception that the definition of “under-served rural or remote community” is too restrictive, with many recipients suggesting the definition should take into consideration not only a community’s size, but also its access to health care. When presented with an alternative definition using Statistics Canada’s term “rural area,” defined as any area outside a population centre, 3 in 10 believed this would more accurately represent under-served rural and remote areas compared to the current definition. The rest of the participants mentioned that ensuring that eligibility was extended to all “rural areas,” as defined by Statistics Canada, would be a great start, but limiting it only to rural areas would be too narrow of a definition. Participants recommended that a new definition should also include smaller population centres.
Prepublication in the Canada Gazette, Part I
The regulatory amendments were prepublished in the Canada Gazette, Part I, on June 29, 2024, followed by a 30-day comment period. A total of five comments were received through the Government of Canada’s Online Regulatory Consultation System. They included one from an anonymous source and one from an individual member of the public. The other comments were from the Canadian Nurses Association, the College of Family Physicians of Canada, and the Canadian Association of Student Financial Aid Administrators.
The anonymous source comment advocated for loan forgiveness to be applied to all student loans, regardless of career path or employment location. The comment from the individual member of the public advocated for recognition and acceptance of foreign medical, nursing and veterinary credentials, and that foreign doctors, nurses and veterinarians should be incentivized to come to Canada. Neither source provided any feedback specific to the regulatory amendments. As both comments are beyond the scope of the regulatory amendments, they did not result in any changes to the regulations.
A comment from the Canadian Nurses Association commended the Government’s initiative to extend the forgiveness benefit to nurses working in all rural communities. It noted that, in a 2022 survey conducted with 2 500 nurses, federal tax incentives were highlighted as one of the top three measures that can help address nursing shortages. The College of Family Physicians of Canada (CFPC) applauded enhancing financial support for family physicians, especially recent graduates, but suggested that reconsideration should be given to growing under-served communities and that retention of physicians should also be a regulatory priority. The Program recognizes that while some under-served communities will outgrow their eligibility for the forgiveness benefit, the provision allowing communities to remain eligible for at least six months after census population results are published was designed to enable communities time to adapt their recruitment strategies to account for the loss of eligibility. In addition, doctors and nurses who begin receiving loan forgiveness in a community will continue to receive it for the full five years even if that community no longer qualifies for the benefit. While the CFPC agrees that the forgiveness benefit is a good initial incentive, it indicated that it is limited with respect to ensuring long-term retention of family physicians. The CFPC also noted that sustainable practice environments will be important for future recruitment and long-term retention in areas that are anticipated to lose their eligibility for loan forgiveness following the 2026 census due to population increases. The Canadian Association of Student Financial Aid Administrators expressed support for the changes, indicating that they make the forgiveness benefit more accessible to doctors and nurses. However, it noted the importance of communicating the changes and that the list of eligible professions should be expanded. While these comments may be considered in the context of future CSFA Program amendments, the amount of the loan forgiveness benefit and the extension of the benefit outside of rural and remote communities are beyond the scope of the present regulatory amendments and, therefore, did not result in any changes to the regulations. As there were no changes to the regulations as a result of prepublication and no comments on the cost-benefit analysis, the cost-benefit assessment remained unchanged.
Modern treaty obligations and Indigenous engagement and consultation
The regulatory amendments are not expected to have differential impacts on Indigenous peoples or negative implications for modern treaties, according to the Government of Canada’s obligations in relation to rights protected by section 35 of the Constitution Act, 1982. The regulatory amendments were assessed for modern treaty implications following the Cabinet Directive on the Federal Approach to Modern Treaty Implementation. The assessment found no immediate impacts on modern treaty obligations.
While engaging on the suite of proposed amendments to the forgiveness benefit in 2022, the Program consulted the Indigenous Physicians Association of Canada (IPAC). IPAC recommended that, while financial incentives would incentivize people to work in rural and remote areas, the focus should be on building the community’s capacity, such as training local residents who are more likely to stay long term in their home communities. In addition, IPAC recommended that resources may be better put towards mitigating barriers for people from rural areas getting into medical school and subsidizing their training and residency in their home areas.
Unfortunately, post-secondary education institution admission policies for medical schools and the curriculum for education and training are outside the purview of the federal government. Nevertheless, while the Program is a program of general application, it particularly supports Indigenous learners by not requiring these borrowers to make the annual fixed student contribution towards education costs and exempting funding received through the Post-Secondary Student Support Program (as well as through the Métis Nation and Inuit Post-Secondary Education strategies) from counting as a resource in the needs assessment that all applicants for Canada student financial assistance undergo.
Instrument choice
Amending the definition of “under-served rural or remote community” for the purpose of determining eligibility to federal loan forgiveness for doctors and nurses in rural and remote communities could not be addressed by means other than regulatory amendments. The Canada Student Financial Assistance Act footnote 13 (CSFAA) and the Canada Student Loans Act footnote 14 (CSLA) only allow for loan forgiveness with the conditions to be prescribed by the related regulations. As a result, non-regulatory options were not considered.
Regulatory analysis
Benefits and costs
A cost-benefit analysis was conducted to assess the incremental impacts of amending the definition of “under-served rural or remote community” for the forgiveness benefit. The cost-benefit analysis was compared to a baseline scenario in which these regulatory amendments are not made. The complete cost-benefit analysis is available upon request.
The stakeholders that will be most directly affected are the residents of the designated rural or remote communities, eligible doctors and nurses with outstanding Canada Student Loans, and the Government of Canada.
The key data source for this cost-benefit analysis is the Program administrative data, specifically the number of recipients and the number of loans forgiven through this benefit, the census 2021 population data, and the Standard Geographical Classification 2011 and 2021. In addition, a review of research literature helped identify the impacts of increased access to health care services for individuals who reside in rural or remote communities, as well as debt forgiveness as a financial incentive for health care providers to move and work in rural communities.
It is anticipated that the change in definition will incentivize 935 doctors and nurses to provide health services to a rural or remote community over a 10-year period (2024–2034), starting with an additional 92 health care professionals in 2024–2025. The increase of 935 beneficiaries for the forgiveness benefit over the 10 years is the net difference between the number of beneficiaries who would have moved to newly eligible rural or remote areas due to the regulatory amendments and the number of beneficiaries who would have moved to an area covered by the previous definition.
By increasing the number of communities eligible for the benefit, the revised definition will also expand the number of residents expected to benefit from better access to health care by approximately 20%, as the increased number of eligible rural and remote communities will increase the number of impacted residents by about 1.7 million from 9.5 million to 11.2 million.
Cost-benefit statement
- Number of years: 10 (2024–2025 to 2033–2034 academic years)
- Base year for costing: 2024
- Present value base year: 2024
- Discount rate: 7% (Canadian Cost-Benefit Analysis Guide: Regulatory Proposals)
Monetized costs
The cost to the Government of Canada for providing loan forgiveness and the cost to Program borrowers who will no longer be eligible for loan forgiveness under the amendments is based on estimates using Program administrative data.
The monetized cost is the cost of providing increased loan forgiveness to beneficiaries and the cost of no longer receiving loan forgiveness for borrowers working and residing in transitional communities. It is estimated that about 935 additional health workers (280 doctors and 655 nurses) will be incentivized by these regulatory amendments; this is the result of an additional 2 120 professionals in newly eligible areas (517 doctors and 1 603 nurses) and the loss of 1 185 professionals (237 doctors and 948 nurses) in transitional areas following the expiration of the transitional provision. The total monetized costs are estimated at $87.4 million (present value) over the next 10 years.
Furthermore, there will be some incremental costs for the Program’s service provider to process and administer loan forgiveness for these additional beneficiaries; however, these costs will not require additional funding, as they are covered by the contract between the service provider and the Government of Canada.
| Impacted stakeholder | Description of cost | Base year 2024–2025 | Second year 2025–2026 | Fifth year 2028–2029 | Final year 2033–2034 | Total (present value) | Annualized value |
|---|---|---|---|---|---|---|---|
| Government of Canada | Cost due to new eligible areas | $3.5 | $7.3 | $8.2 | $10.0 | $58.6 | $8.3 |
| Program borrowers | Ineligibility of loan forgiveness in transitional areas | $0.0 | $0.0 | $4.8 | $8.2 | $28.8 | $4.1 |
| All stakeholders | Total costs | $3.5 | $7.3 | $13.1 | $18.2 | $87.4 | $12.4 |
Monetized benefits
The regulatory amendments will provide an incentive for specified health care professionals to work in newly eligible rural and remote communities and savings for the Government of Canada due to some areas being no longer eligible once the transitional provisions expire. These benefits were monetized by attributing the equivalent estimated costs incurred by the Government for loan forgiveness as a benefit to the borrowers in the newly eligible rural areas. Similarly, the loss of loan forgiveness beneficiaries in transitional areas becomes a benefit to the federal government in terms of loan forgiveness savings due to the amendments. The total monetized benefits are estimated at $87.4 million (present value) over the next 10 years.
| Impacted stakeholder | Description of benefit | Base year 2024–2025 | Second year 2025–2026 | Fifth year 2028–2029 | Final year 2033–2034 | Total (present value) | Annualized value |
|---|---|---|---|---|---|---|---|
| Government of Canada | Savings due to transitional areas ineligibility to receive benefit | $0.0 | $0.0 | $4.8 | $8.2 | $28.8 | $4.1 |
| Program borrowers | Benefit due to new areas eligible | $3.5 | $7.3 | $8.2 | $10.0 | $58.6 | $8.3 |
| All stakeholders | Total costs | $3.5 | $7.3 | $13.1 | $18.2 | $87.4 | $12.4 |
The regulatory amendments will forgive the federal student debt of doctors and nurses who work in rural or remote communities. Research demonstrates that loan forgiveness and loan repayment programs are strong incentives that may influence medical residents’ career choices and recommend financial incentives that reward physicians who provide care to at-risk populations.footnote 15 Doctors and nurses have significant federal debt loads when compared to the average Program client. This is especially true for family physicians who utilize the forgiveness benefit, as they have more than double the Canada Student Loan debt when compared to the average Program client.
The regulatory amendments will also allow these borrowers to repay their loans faster. This will enable them to service other educational and non-educational debt, increase their savings and have increased disposable income. Research demonstrates that having a high level of student debt is directly linked to financial difficulties and hardship, even for individuals who manage to make regular payments.footnote 16 In terms of medical student debt, individuals with higher amounts of student loan debt were more likely to report high levels of stress from their educational debt and are more likely to delay major life decisions, such as getting married, having children and buying a house.footnote 17
| Impacts | First year 2024–2025 | Second year 2025–2026 | Fifth year 2028–2029 | Final year 2033–2034 | Total (present value) | Annualized value |
|---|---|---|---|---|---|---|
| Total benefits | $3.5 | $7.3 | $13.1 | $18.2 | $87.4 | $12.4 |
| Total costs | $3.5 | $7.3 | $13.1 | $18.2 | $87.4 | $12.4 |
| NET IMPACT | $0 | $0 | $0 | $0 | $0 | $0 |
Quantified impacts
The regulatory amendments are expected to increase the number of doctors and nurses working in rural or remote communities.
| Impacts | First year 2024–2025 | Second year 2025–2026 | Fifth year 2028–2029 | Final year 2033–2034 | Total |
|---|---|---|---|---|---|
| Number of doctors incentivized to provide health services in rural or remote communities due to CSL forgiveness | 22 | 47 | 25 | 22 | 280 |
| Number of nurses incentivized to provide health services in rural or remote communities due to CSL forgiveness | 70 | 145 | 61 | 23 | 655 |
| Total incremental number of doctors and nurses in rural and remote communities that will benefit from the amendments | 92 | 192 | 86 | 45 | 935 |
While there are many reasons for doctors and nurses to work in rural or remote areas, research demonstrates that monetary incentives are an important factor in recruiting doctors and nurses to these communities.footnote 18,footnote 19 Research also demonstrates that providing financial incentives has allowed communities to strategically recruit health care providers and that financial incentives have a positive effect on the recruitment of doctors and nurses when compared to communities that did not provide financial incentives.footnote 20,footnote 19
Qualitative impacts
Increasing the number of health care providers working in rural or remote communities is expected to help improve access to health care services. Rural or remote communities face unique challenges across the various social determinants of health.footnote 21 In particular, lack of access to health care providers results in unmet health care needs, including lack of preventive and screening services, and treatment of illnesses. Access to a regular primary health care provider is generally associated with better health outcomes, and providing local access to health care helps address the health problems of the local population.footnote 22,footnote 23 Furthermore, research demonstrates that communities with populations above 30 000 typically have a broader scope of health care services compared to smaller communities, and residents have to travel shorter distances to access health care services compared to smaller communities.footnote 24 By increasing incentives for doctors and nurses to work in rural or remote communities, the regulatory amendments will result in better health care services and continuity of care. Initially, these regulatory amendments are expected to increase the availability of health care services for approximately 1.7 million Canadians living in newly eligible areas.
About 1.1 million Canadians reside in areas that will remain eligible under the transitional provision until census 2026, at which time those areas will become ineligible for the forgiveness benefit. This will lead to an initial net incremental increase of about 640 000 more people living in areas where doctors and nurses are eligible for the forgiveness benefit. These population count estimates only reflect the areas affected by the regulatory amendments and do not consider the possibility that some doctors and nurses may continue to serve in communities that become ineligible for a period after the changes are implemented.
The literature examined suggests that the increased number of doctors and nurses in rural or remote regions could have an influence on health indicators. Research from the United States shows that increasing the supply of primary care physicians by one unit per 10 000 population is associated with improved health outcomes in the range of 0.66% to 10.8% and an average mortality reduction of 5.3%.footnote 25 Similarly, research on Canadian health expenditures finds that increases in health spending can positively impact a variety of health indicators.footnote 26
After the transitional provision expires, some communities will become ineligible for the forgiveness benefit. However, these communities may not necessarily lose their health care professionals. Financial incentives are one of the many reasons why health care professionals may move to rural communities; other incentives include rural background and preference, quality of life, professional support and experience, clinical placements, and autonomy in practice.footnote 20 Furthermore, the forgiveness benefit survey of recipients found that about two thirds of doctors and 7 in 10 nurses continued to practise in an under-served rural or remote community in 2019–2020 without being eligible for the benefit. Therefore, even if the financial incentive no longer exists for some communities, previous recipients may remain in those communities.
Moreover, this measure’s aim is to improve accessibility for individuals residing in under-served rural or remote communities who have more limited access to primary care than individuals in urban settings. As population size increases in a community, research demonstrates that health and primary care access improves.footnote 27,footnote 28
The monetized benefits exclude qualitative benefits to Canadians living in rural or remote communities and Canadian society, such as improved access to health services and, as suggested by the evidence in the literature reviewed, better health outcomes. As a result, the benefits of implementing the regulatory amendments likely outweigh the costs.
Small business lens
Analysis under the small business lens concluded the regulatory amendments will not impact Canadian small businesses.
One-for-one rule
The one-for-one rule does not apply to these regulatory amendments, as there is no change in the administrative burden on businesses.
Regulatory cooperation and alignment
The regulatory amendments are not related to any commitment under a formal regulatory cooperation forum. The Program has consulted with P/T stakeholders, and they have been supportive of the measures. In addition, while Quebec, Nunavut and the Northwest Territories do not currently participate in the Program, they could still benefit from the forgiveness benefit for doctors and nurses. Eligible health professionals who received a Canada Student Loan in a participating P/T are still permitted to benefit from loan forgiveness if they worked in an under-served rural or remote community in Quebec, Nunavut or the Northwest Territories.
Amending the definition of “under-served rural or remote community” in the context of the forgiveness benefit is aligned with P/T strategies to increase health care capacity in rural and remote communities. In 2023 provincial budgets, Albertafootnote 29 and Saskatchewanfootnote 30 each committed to making significant investments in the recruitment and retention of physicians and nurses in rural and remote areas.
In addition, the provinces of Saskatchewan and British Columbia have loan forgiveness programs in place that target health professions. Manitoba, Ontario, and Newfoundland and Labrador have grant and bursary programs aimed at health care graduates:
- Under Saskatchewan’s loan forgiveness program, nurses and nurse practitioners receive forgiveness of one fifth (20%) of their outstanding Saskatchewan student loan debt, up to $4,000 annually, for up to five years, to a maximum of $20,000. Eligible communities in Saskatchewan must also have a population of fewer than 10 000, with the exception of eight select communities,footnote 31 with populations greater than 10 000 that are also included. This is a much more restrictive threshold than the federal forgiveness benefit.
- British Columbia’s loan forgiveness program forgives student loan debt for eligible professionals working in an under-served community to a maximum of 20% of the provincial portion of a Canada-British Columbia integrated student loan, for up to five years. Under British Columbia’s program, eligible occupations include nurses and physicians, as well as other professions, such as midwifery, occupational therapy, physiotherapy and respiratory therapy. In addition, loan forgiveness is available to certain occupations that work with children, such as school psychologists and teachers of the deaf, hard of hearing or visually impaired.
- Manitoba’s Grant for Nursing Graduates provides $4,000 (or $8,000 if working in a care home) to eligible graduates of a nursing program in Manitoba who agree to serve for at least 12 months in any community in Manitoba, outside of Winnipeg or Brandon.
- Ontario’s Learn and Stay grant provides free tuition for students in eligible programs, including undergraduate and postgraduate degrees in nursing, and diploma programs in practical nursing, paramedics, and medical laboratory science. Such students must commit to fulfilling a service agreement to work in the same region in which they studied after graduation, for at least six months for every full year of study.
- Newfoundland and Labrador’s Medical Resident Bursary provides a one-time funding amount to medical residents practising in designated areas of need in the province. Applicants must agree to practise for 36 months in a full-time position at a specific location upon obtaining full licensure. Four funding levels have been assigned to communities based on level of rural location and remoteness. Bursary amounts increase for more rural and difficult-to-fill positions, from a minimum of $25,000 to a maximum of $90,000.
Meanwhile, several P/Ts, such as Nova Scotia, Prince Edward Island, Quebec, Nunavut and the Northwest Territories, also offer broad loan forgiveness programs not targeted at specific occupations.
Effects on the environment
In accordance with the Cabinet Directive on Strategic Environmental and Economic Assessment, a preliminary scan concluded a strategic environmental assessment is not required.
Gender-based analysis plus
The regulatory amendments support eligible borrowers and, in a broader sense, the greater Canadian population. The gender-based analysis plus (GBA+) did not identify any unintended adverse, disproportionate or differential impacts resulting from the regulatory amendments.
Changing the definition of “under-served rural or remote community” is expected to make more rural and remote communities eligible for the benefit, as the previous definition excluded some communities located at a commuting distance from larger urban centres. Rural and remote communities have historically faced barriers to health care access, including a shortage of primary care providers, increased travel time to health care facilities and economic hardship. Research finds that rural populations are less likely to have access to a regular health care provider or visiting specialists.footnote 32 Moreover, Statistics Canada data shows that treatable mortality rates increased as remoteness increased for both males and females.footnote 33 Higher preventable and treatable mortality rates in the remote areas could be attributed to geographic barriers, limited health care services, and unmet health care needs.footnote 33 For example, the treatable mortality rate for easily accessible areas was 71.4 deaths per 100 000 population for men and 61.2 deaths per 100 000 population for women. In comparison, for remote areas, this rate is 89.2 deaths per 100 000 population for men and 76.0 deaths per 100 000 population for women.
Program data indicates that forgiveness beneficiaries are typically between the ages of 18 to 29 years old. According to Program data, 74% of individuals with outstanding Canada Student Loans are under 35 years of age. Literature examined suggests that financial incentives can play a greater role in motivating younger physicians (i.e. younger than 45 years of age) to move to a rural area than in the case of older physicians.footnote 34 Therefore, the regulatory amendments are expected to benefit more borrowers under the age of 35 compared to other age groups, as these beneficiaries are more likely to be repaying their loans and more likely to be influenced by financial incentives than older physicians.
As a majority of the current loan forgiveness beneficiaries are women, the Program expects that expanding the definition of a rural or remote community will particularly benefit women working as eligible professionals under the Program. In 2021–2022, 83% of forgiveness benefit recipients were female and Program data from the same year found 89% of nurses receiving the forgiveness benefit were women. In 2021–2022, doctors only made up about 18% of loan forgiveness recipients; 56% of those doctors were women.
Implementation, compliance and enforcement, and service standards
Implementation
The regulatory amendments will come into force upon publication.
Once the regulatory amendments are in force, the revised definition will be applicable to a qualifying health professional who has completed a year of work. For example, if the regulatory amendments come into force on November 1, 2024, a qualifying health professional will be eligible for the benefit if they started a year of work in an under-served rural or remote community on or after November 1, 2023.
The way in which eligibility for the forgiveness benefit is assessed will remain unchanged. The applicant provides a postal code for the facility/facilities where they have worked, which is attested to by the employer or by a local official in the case of a self-employed individual. Program officers then compare the postal code provided by the applicant against the list of postal codes of identified under-served rural or remote communities.
Existing F-P/T and stakeholder fora will be used to notify all stakeholders of the changes.
The effect of the changes to the forgiveness benefit will be incorporated into existing performance measurement and evaluation mechanisms. Employment and Social Development Canada’s (ESDC) Evaluation Directorate recently completed an evaluation of the Program in March 2021.footnote 35 In addition, ESDC’s Evaluation Directorate recently completed an evaluation of the forgiveness benefit, released on January 22, 2024.footnote 36
Compliance and enforcement
The Canada Student Financial Assistance Act (CSFAA) requires the Program to table an actuarial report in Parliament at least once every three years. This report provides an estimate of Program costs and revenues, a 25-year forecast of future Program costs and revenues, and an explanation of the methodology and actuarial and economic assumptions used to produce the figures presented in the report. The CSFAA also requires an annual report on the Program to be tabled in Parliament. The report provides detailed Program statistics (including the value of the portfolio) and outlines key objectives, initiatives, and accomplishments achieved over a given academic year as well as the integrity policies.footnote 37
The CSFAA provides authority for the Program to ensure that federal grants and loans are not provided to students who are not eligible. Subsection 17(1) of the CSFAA provides for a fine of up to $1,000 for students who knowingly provide any false or misleading information, including by omission, in an application or other document. Also, section 17.1 of the CSFAA allows for any such student to be denied additional federal financial assistance, as well as certain other Program benefits, such as repayment assistance.
Contact
Erin Hetherington
Director
Program Policy Division
Canada Student Financial Assistance Program
Learning Branch
Employment and Social Development Canada
200 Montcalm Street, Tower II, 7th Floor
Gatineau, Quebec
J8Y 3B5
Email: EDSC.DGA.PCAFE.MCPP-SEC.CSFAP.LB.ESDC@hrsdc-rhdcc.gc.ca